Piercing Bump vs Keloid: How to Tell the Difference Fast
What Is a Piercing Bump? (The Common Culprits)
A piercing bump is a small, raised area of skin that forms at the site of a healing piercing, commonly caused by irritation, trapped fluid, mild infection, or a localized excess of scar tissue known as hypertrophic scarring. Most people who discover a bump near their piercing are dealing with one of three types:
Irritation bump: The most common. This forms when the piercing is repeatedly disturbed — sleeping on it, snagging on clothing, over-cleaning, or using jewelry that’s too short or made from reactive metals. It presents as a small, reddish, slightly moist bump directly at the entry or exit hole. It may have a thin crust of dried lymph fluid and can feel tender to the touch. It is not pus-filled unless a secondary bacterial infection has developed.
Pustule: A small, fluid- or pus-filled bump caused by a mild infection or a reaction to an irritant. Pustules feel soft, may have a yellowish center, and are usually no larger than a few millimeters. They differ from true abscesses, which involve deeper, more significant infection and require medical attention.
Hypertrophic scar: A firm, pink, raised scar that stays within the boundaries of the piercing channel. Hypertrophic scars involve excess collagen production during wound healing, but unlike keloids, they do not invade surrounding tissue. They’re more common at cartilage piercings and can persist for months. According to StatPearls (NCBI), hypertrophic scars may undergo partial spontaneous resolution over time — something keloids rarely do.
Common triggers include sleeping on a new cartilage piercing, wearing jewelry with a nickel alloy (a frequent allergen), over-cleaning with alcohol or hydrogen peroxide, and poor initial jewelry fit (too tight or too short).
What Is a Keloid? (The Real Deal)
A keloid is an overgrowth of scar tissue that extends beyond the boundaries of the original wound, forming a smooth, shiny, raised mass that can be pink, red, purple, or significantly darker than the surrounding skin. Unlike a hypertrophic scar that stays confined to the wound site, a keloid invades the neighboring skin, often making the original piercing hole difficult to locate beneath the mass.
Keloids are a genetically influenced condition. Research published in dermatology literature consistently indicates that keloid formation is more common in people of African, Asian, Hispanic, and Mediterranean descent, with some studies suggesting the incidence may be up to 15 times higher in darker-skinned populations compared to lighter-skinned populations. If a close family member has a history of keloids, your risk increases substantially.
Keloids do not regress on their own. They can continue growing for months or even years after the original piercing, and they will not respond to any home remedy or aftercare adjustment. Their defining characteristic — invasive growth beyond the wound margin — is what separates them from every other type of piercing bump.
If you’ve had keloids from any prior wound, surgery, or piercing, dermatologists universally advise against new piercings in high-risk locations such as the ear cartilage, chest, and shoulders. This is critical information that many aftercare guides omit.
Piercing Bump vs Keloid: 7 Key Differences
The difference between a piercing bump and a keloid comes down to location, growth pattern, texture, and whether the bump responds to standard care. Study the table below, then cross-reference with the written descriptions that follow.
| Feature | Piercing Bump (Irritation / Hypertrophic) | Keloid |
|---|---|---|
| Location | At the piercing exit hole; sits on entry/exit point | Extends well beyond the piercing site into surrounding skin |
| Shape | Small, round, or slightly elongated; follows the piercing channel | Irregular, dome-shaped, or elongated; grows outside wound margins |
| Texture | Soft or slightly firm; may ooze fluid or have a dried crust | Firm, rubbery, smooth; no discharge |
| Color | Red, pink, or flesh-toned; may have a yellowish fluid center | Pink, red, purple, or dark brown; uniform smooth surface |
| Growth Pattern | Appears within weeks; may fluctuate in size; often shrinks with corrected care | Grows slowly over months to years; rarely regresses spontaneously |
| Pain / Itch | Mild tenderness or soreness; occasional itching | Can be intensely itchy, tender, or painful as scar tissue stretches |
| Response to Treatment | Improves with saline soaks, jewelry upgrade, or time | Requires medical treatment (steroid injections, laser, cryotherapy, excision) |
Location matters most. Run a clean fingertip around the bump. An irritation bump has a clear relationship to the piercing hole — you can feel where the hole is beneath it. A keloid feels like a separate, freestanding mass that has swallowed the surrounding area.
Growth pattern is the decisive test over time. An irritation bump may flare up and calm down across weeks. A keloid moves in one direction: outward and upward. If your bump has measurably grown over 6–8 weeks despite correct aftercare, that is the clearest signal that a dermatologist visit is no longer optional.
Texture confirms the diagnosis. A keloid is characteristically firm and rubbery — distinctly different from the soft, sometimes fluctuant feel of an irritation bump or the moderately firm feel of a hypertrophic scar.
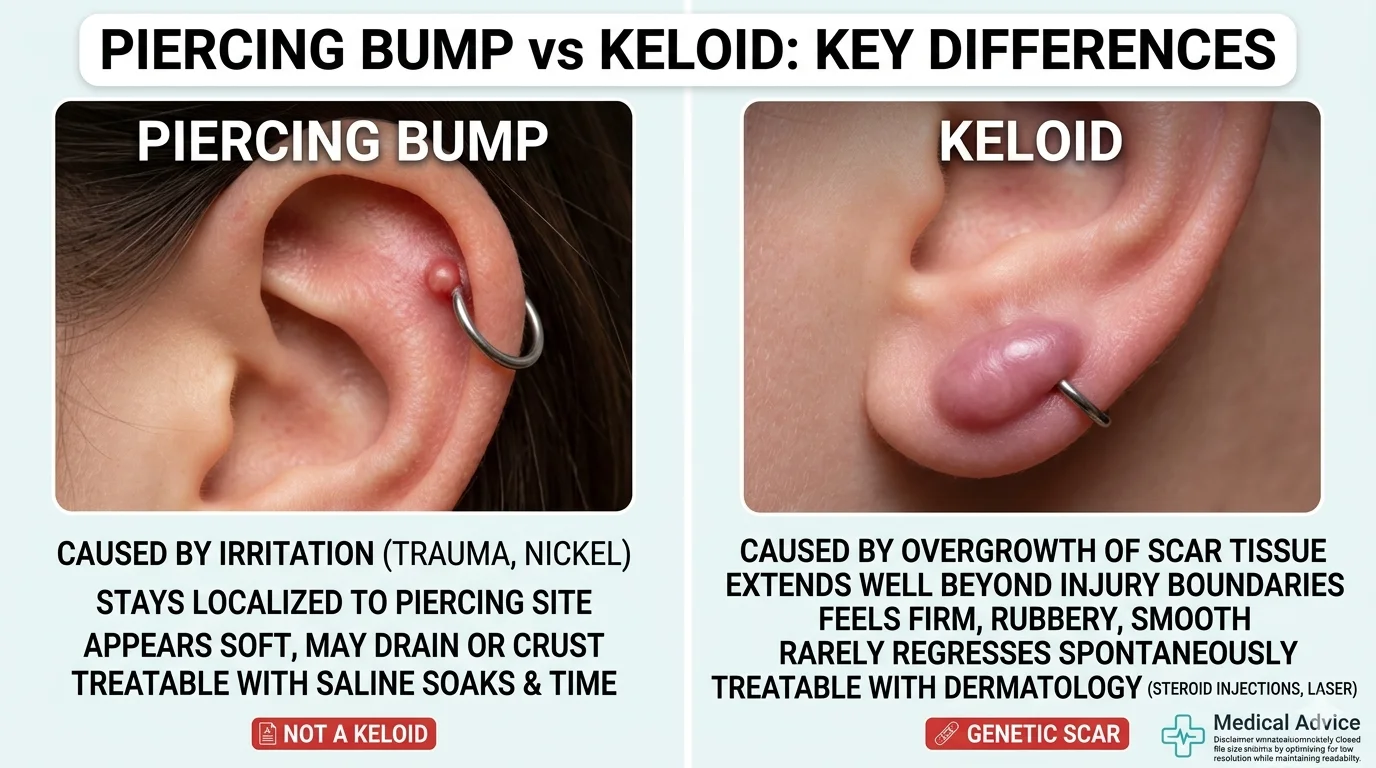
Visual Guide: How to Spot a Keloid vs an Irritation Bump
Picture this: an irritation bump looks like a small, angry pimple sitting directly on the piercing hole. It may have a slight red ring, a tiny crusty cap of dried lymph fluid, and a soft center. If you have a nostril stud, you’ll see the bump right where the post exits — the jewelry is still visible and sitting normally.
A keloid looks fundamentally different. It’s a smooth, rubbery lump that has effectively engulfed the piercing area. The jewelry may sit unevenly or appear partially buried within the scar mass. On an earlobe, a keloid can grow on both the front and back of the ear simultaneously, forming a dumbbell shape around the lobe. On ear cartilage, it can spread across the helix in a band.
Piercing locations most prone to keloids: Ear cartilage (helix, tragus, daith), earlobes in keloid-prone individuals, chest/sternum, nape of the neck, shoulders, and upper back. These areas have higher skin tension and more reactive collagen responses.
Piercing locations more commonly associated with irritation bumps: Nostril, navel, eyebrow, and oral piercings. These sites still carry some keloid risk in predisposed individuals, but the overwhelming majority of bumps there are irritation-related.
What Causes a Piercing Bump to Form?
Piercing bumps are not a sign of failure or unclean habits — they are a normal inflammatory response that becomes disproportionate when the piercing is irritated. The most common causes:
Mechanical trauma is the leading culprit. Sleeping on a new cartilage piercing without a travel pillow, catching the jewelry on a hairbrush, or bumping a fresh nostril stud compress and twist the healing fistula (the skin channel forming around the jewelry), triggering the body to produce excess fluid and inflammatory cells.
Wrong jewelry material. Reactive metals — particularly alloys containing nickel — can cause contact dermatitis at the piercing site. The Association of Professional Piercers (APP) recommends implant-grade titanium (ASTM F136), implant-grade steel (ASTM F138), solid 14k or 18k gold, or niobium for initial piercings. Surgical steel is not the same standard.
Harsh cleaning products. Alcohol, hydrogen peroxide, iodine-based products (Betadine), and antibacterial soaps disrupt the healing tissue, kill beneficial skin flora, and cause chemical micro-irritation. Both the APP and Mayo Clinic recommend avoiding all of these during piercing healing.
Over-cleaning or under-cleaning. Cleaning more than twice a day is itself a source of irritation. Conversely, not cleaning at all allows debris and bacteria to accumulate.
Jewelry that is too short or too tight. Jewelry that presses the disc or ball tightly against the skin causes embedded pressure, restricting blood flow and triggering a localized inflammatory response.
What Causes a Keloid to Form on a Piercing?
Keloids represent an aberrant wound-healing response — the body’s collagen-producing fibroblasts fail to receive the chemical signal to stop, leading to unchecked scar tissue growth. The exact mechanism is not fully understood, but research points to several established risk factors:
Genetic predisposition is the most significant. Keloid scarring is strongly associated with inherited traits, particularly among those with higher melanin content in their skin. According to Dermatology Advisor, African-American, Asian, Hispanic, and Mediterranean populations carry elevated risk. If a parent or sibling has keloids, consider that a significant personal risk factor before getting cartilage or chest piercings.
Location and skin tension. Ear cartilage is the single most common site for keloids from piercings. Cartilage has a poor blood supply, heals more slowly, and the curved surface creates mechanical tension on the healing wound — all conditions that promote keloid formation.
Piercing guns vs. needles. The APP warns that reusable piercing guns cannot be properly sterilized and cause blunt-force trauma to cartilage that needles do not. The additional tissue damage from a gun increases keloid risk in predisposed individuals.
Delay in treatment. A hypertrophic scar left without intervention can, in some genetically predisposed individuals, transition toward keloid behavior. Early correction of irritants and prompt dermatological evaluation if growth continues is important.
Treatment Options: How to Get Rid of a Piercing Bump
If you have an irritation bump or hypertrophic scar, the goal is simple: remove the source of irritation and allow the piercing to heal undisturbed.
Daily Aftercare Routine (APP-Aligned)
| Step | Action | Notes |
|---|---|---|
| Morning | Spray sterile saline (0.9% sodium chloride wound wash) onto the piercing | Do not use homemade salt solutions; the APP no longer recommends them |
| After shower | Let the shower water rinse the piercing naturally; pat dry with clean disposable gauze | Never use cloth towels — fibers snag jewelry and harbor bacteria |
| Evening | One additional saline spray if needed | Less is more; over-cleaning delays healing |
| Ongoing | Leave the jewelry completely alone | No rotating, no twisting, no touching with unwashed hands |
Switch your jewelry. If you have any doubt about the material, visit an APP-certified piercer and ask for a downsize to implant-grade ASTM F136 titanium. Many bumps resolve entirely after a jewelry upgrade.
LITHA (Leave It The Hell Alone). This evidence-aligned philosophy — endorsed by professional piercers and consistent with APP guidance — holds that the body’s natural healing mechanisms are efficient, and constant touching, rotating, and product application does more harm than good. Saline once or twice a day, then leave it entirely alone.
Warm compresses. For stubborn irritation bumps, warm (not hot) saline compresses applied for 5 minutes help increase blood circulation to the area, reduce inflammation, and encourage fluid drainage.
See a professional when: There is no improvement after 2–4 weeks of corrected care; the bump is growing; there is spreading redness, warmth, red streaks extending from the site, or fever (signs of infection requiring antibiotic treatment, not just saline). The APP also notes that removing jewelry in the presence of an active infection can trap bacteria and worsen the situation — leave the jewelry in and see a doctor.
Treatment Options: How to Treat a True Keloid
Keloid treatment is a medical matter. There is no home remedy that reliably reduces a true keloid — tea tree oil, aspirin paste, and apple cider vinegar are not clinically validated treatments and carry a risk of skin damage.
Corticosteroid injections (first-line treatment). Intralesional triamcinolone acetonide injections, administered by a dermatologist every 4–6 weeks, remain the gold standard for keloid management. The steroid reduces collagen synthesis within the scar and can flatten the keloid over a series of sessions. Response rates vary; multiple injections are typically required.
Silicone gel sheets. Applied daily to the scar surface, medical-grade silicone sheets (not generic scar creams) create a hydrated, low-oxygen microenvironment that suppresses scar activity. Best used early and consistently over 2–3 months; also useful as adjuvant therapy following injections.
Cryotherapy. Liquid nitrogen applied to the keloid destroys abnormal scar tissue cells. More effective on smaller keloids. May cause temporary hypopigmentation, particularly important to discuss for darker skin tones.
Laser therapy. Pulsed dye laser (PDL) targets the vascular component of keloids, reducing redness and bulk. Fractional laser combined with intralesional steroid delivery (laser-assisted corticosteroid delivery) has shown improved outcomes in dermatology research over standalone injections.
5-Fluorouracil (5-FU) injections. This chemotherapy agent, injected intralesionally alone or in combination with triamcinolone, inhibits fibroblast proliferation. The combination protocol is increasingly used for keloids resistant to steroid monotherapy.
Surgical excision. Removing the keloid with a scalpel carries a high recurrence risk if not paired with immediate post-surgical adjuvant therapy (radiation, pressure garments, or corticosteroid injections). Excision alone — without adjuvant treatment — has recurrence rates reported as high as 80%.
Critical warning: Never attempt to cut, pop, or excise a keloid at home. The physical trauma of the attempt will almost certainly trigger a larger, more aggressive keloid regrowth. Keloid formation is driven by the same wound-healing process — amplified — that would respond to any new skin injury.
Can You Pop a Piercing Bump?
No. Popping a piercing bump introduces external bacteria into a healing wound channel, worsens inflammation, can rupture the fistula wall internally, and significantly increases the risk of infection. An infected bump is harder to treat, slower to heal, and more likely to result in permanent scarring than one left alone. Even if fluid comes out temporarily, the underlying cause (irritation, excess fluid production, or early hypertrophic scarring) remains unchanged — and the newly opened wound creates additional trauma. Resist the urge entirely.
Common Myths About Piercing Bumps and Keloids
Myth: “Rotating my jewelry prevents it from getting stuck.” This is one of the most persistent and damaging pieces of outdated advice in piercing. Rotating jewelry tears the newly forming fistula tissue every single time. The dried crust around a healing piercing is lymph fluid, not adhesion — the jewelry will not fuse to your skin. Stop rotating.
Myth: “Tea tree oil cures piercing bumps.” Tea tree oil is an essential oil that can cause chemical burns on broken skin. It has no role in evidence-based piercing aftercare.
Myth: “If it’s not a keloid, I don’t need to do anything.” Irritation bumps left untreated — with the irritating cause still in place — can evolve into stubborn hypertrophic scars and, in genetically predisposed individuals, can progress toward keloid behavior. Correcting the cause matters.
Myth: “Keloids only happen to people with dark skin.” Keloids occur across all skin tones, but the prevalence is statistically higher in individuals with more skin melanin. Anyone can develop a keloid. No one is immune.
Myth: “If I’ve had a piercing before without a keloid, I’m safe.” Keloid risk can vary by location. A person with no keloid history on their earlobes may develop one on cartilage due to the physiological differences in that tissue and the higher mechanical tension.
Piercing Aftercare: Preventing Bumps and Keloids Before They Start
Prevention is always more effective than treatment. Here’s what the evidence supports:
Choose an APP-certified piercer. The APP sets standardized aftercare and jewelry protocols that measurably reduce complication rates. Find a member at safepiercing.org.
Start with implant-grade jewelry. ASTM F136 titanium, solid 14k/18k gold, or niobium have the lowest rates of contact allergy. Request implant-grade material, not just “surgical” steel.
Follow the APP’s saline-only aftercare. Use a sterile wound wash with 0.9% sodium chloride as the only active ingredient. Spray once or twice a day; do not soak in homemade solutions; avoid all other products.
Protect the piercing from mechanical trauma. Use a travel pillow with a center hole when sleeping on a new ear piercing. Keep hair products away from fresh piercings. Avoid tight clothing over navel or surface piercings.
If you’re keloid-prone: Discuss your history openly with your piercer and a dermatologist before proceeding. Consider pressure earrings (AfterCare earrings or similar devices) for earlobe piercings to minimize the scar response. Avoid ear cartilage, chest, and back piercings — these carry the highest keloid risk in predisposed individuals.
Glossary of Key Terms
Fistula: The skin tunnel that forms around jewelry during piercing healing. Hypertrophic scar: Excess scar tissue confined within the wound boundary; can regress partially over time. Keloid: Abnormal scar tissue extending beyond wound boundaries; does not regress without medical intervention. Intralesional injection: A medical injection administered directly into the lesion (e.g., triamcinolone into a keloid). Triamcinolone acetonide: A corticosteroid used as first-line medical treatment for keloids. Pyogenic granuloma: A vascular overgrowth of granulation tissue; sometimes mistaken for a piercing bump; appears as a moist, bright red, easily bleeding lump. Contact dermatitis: An inflammatory skin reaction triggered by contact with an allergen (such as nickel in jewelry alloys). Implant-grade titanium: ASTM F136 titanium — the biocompatible standard for initial piercing jewelry as recommended by the APP. LITHA: “Leave It The Hell Alone” — a minimal-intervention aftercare philosophy consistent with APP guidelines.
Frequently Asked Questions
Can a piercing bump turn into a keloid? An irritation bump does not directly “turn into” a keloid. However, in individuals with a genetic predisposition, chronic unresolved scar tissue at a piercing site can evolve toward keloid behavior over time. If your bump has been growing for months and not responding to corrected aftercare, dermatological evaluation is important.
How long does it take for a pierced lump to disappear? Irritation bumps typically resolve within 2–8 weeks once the irritating cause is removed and proper saline aftercare is in place. Hypertrophic scars take longer — often 3–12 months — and may not disappear entirely without professional intervention. The APP notes that cartilage piercings can take 6–18 months to fully heal; bumps within that window may still resolve naturally.
What does a keloid on a piercing look like? A keloid looks like a smooth, firm, dome-shaped or irregularly shaped scar that extends beyond the original piercing hole. It may be pink, red, purple, or darker than the surrounding skin. The jewelry often sits unevenly or appears partially buried within the mass. On earlobes, keloids may form on both front and back simultaneously.
Are keloids from piercings permanent? Without treatment, yes — keloids do not resolve spontaneously. With medical treatment (corticosteroid injections, laser therapy, cryotherapy, or surgical excision combined with adjuvant therapy), keloids can be significantly reduced or flattened, though recurrence rates are high. Keloid management is ongoing rather than a single-procedure cure.
Can I still keep my piercing if I have a keloid? This depends on the keloid’s size and location and should be determined with a dermatologist. In many cases, the jewelry must be removed to allow dermatological treatment to be effective, and the piercing channel may scar over permanently. In some milder cases, treatment can proceed with jewelry in place. There is no universal answer — a professional assessment is required.
How quickly can a piercing bump be removed? For an irritation bump: switch to implant-grade titanium jewelry, clean once or twice a day with sterile saline wound wash (0.9% sodium chloride), remove any source of mechanical irritation, and leave it entirely alone the rest of the time. Most irritation bumps respond within 2–4 weeks of this protocol. For a hypertrophic scar, the same approach applies with more patience. For a keloid, no home method is effective — schedule a dermatologist consultation for corticosteroid injections.
Conclusion
The difference between a piercing bump and a keloid is meaningful — one typically resolves on its own with corrected care; the other requires dermatological intervention. Most bumps that appear within weeks of a new piercing are irritation bumps or early hypertrophic scars responding to a specific, correctable cause. A true keloid is firmer, grows beyond the wound site, appears more slowly, and will not shrink without treatment.
If the bump you’re looking at is soft, sits directly on the piercing hole, and appeared within a few weeks of irritation, start with sterile saline aftercare, eliminate the irritant, and give it 4–6 weeks. If the bump is firm, rubbery, growing over months, or extending beyond the piercing site, book an appointment with a board-certified dermatologist. Earlier treatment produces better outcomes.
If you’re still unsure, the safest next step is a 5-minute check-in with an APP-certified piercer — they see these cases daily and can give you an in-person assessment at no cost, often before you need the dermatologist at all.